Trauma Relief Unlimited
T.R.U. Method Effectiveness Report
Compiled and written by Lynne A. Fontaine, Ph.D. with assistance from Robert M. Cicione, LICSW.
This research study examines the effectiveness of the T.R.U. treatment method in reducing the symptoms associated with post-traumatic stress disorder in adults. It also attempts to ascertain if another therapist trained in the T.R.U. method can deliver the treatment. It is hypothesized that the T.R.U. method will reduce the frequency of post-traumatic stress symptoms.
Participants
Forty adults were recruited for participation in this study through advertisements in local newspapers and referrals from helping professionals. Subjects were screened by a T.R.U. therapist and potential subjects were excluded if they had persistent drug and/or alcohol abuse. Upon recruitment, subjects were randomly assigned to one of two groups. The first group would begin the treatment program immediately and the second group waited approximately one month before beginning the program. Scheduling conflicts restricted the ability to have equal numbers in each group, therefore 25 individuals comprised the first group and 15 individuals comprised the second group. Three subjects in the second group did not undergo treatment. The N for the final comparative analyses was 37.
Procedure
Two T.R.U. therapists provided the treatment to the first group. The treatment of the second group was conducted by one of the aforementioned therapists. Each participant was individually evaluated by a T.R.U. therapist prior to beginning the treatment program. Baseline data regarding subject's PTSD symptomatology was collected at this pre-treatment evaluation. Since the first group began their treatment immediately, following their initial evaluation, a T.R.U. therapist treated these subjects for three sessions. Pilot data on the T.R.U. project has shown that three treatment sessions significantly reduces PTSD symptomatology (Cicione, 2000). At each treatment session, the frequency of PTSD symptoms was collected. Following treatment, subjects came in for a post treatment visit and data regarding PTSD symptomatology was collected. Each of the visits occurred approximately one week apart. Subjects in the second group followed the same protocol, yet, since they had a waiting period of one month before beginning treatment, these subjects had essentially two baseline data collection points. For this group, there was no significant difference between the initial evaluation and the baseline evaluation before treatment. To keep data collection points standard between the two groups, the baseline evaluation just before treatment was used in subsequent analyses.
Measures
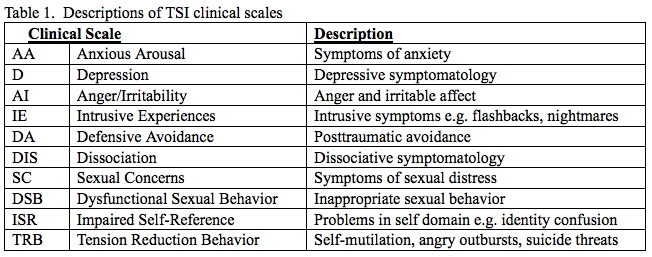
Trauma Symptom Inventory. Each subject completed the Trauma Symptom Inventory (TSI) at the baseline evaluation and at the post-treatment visit. The TSI is a 100 item self-report questionnaire that reflects post-traumatic distress and related psychological symptomatology. The TSI yields ten clinical scales and three validity scales. Only the clinical scales were used in this study (see Table 1). A T-score can be obtained for each clinical scale. A T-score is a standard score that provides information about an individual's score relative to the scores of the subjects in the standardization sample. T-scores have a mean of 50 and a standard deviation of 10, therefore a T-score between 40-60 is considered average. The TSI uses 65 as a clinically significant cutoff score. The TSI has established psychometric properties which are provided in the TSI Professional Manual (Briere, 1995).
Table 1. Descriptions of TSI clinical scales
Clinical Interview
A clinical interview was conducted as part of the initial intake evaluation, prior to each treatment session, and at the post-treatment visit. Subjects indicated the frequency of symptoms such as violent episodes, angry outbursts, nightmares, flashbacks, anxiety attacks, and crying spells. Frequencies were reported in terms of the number of times per week that the particular symptom was experienced. Clinicians also rated the subject's level of depression on a 1-5 Likert type scale with 5 indicating a high level of depression.
Results
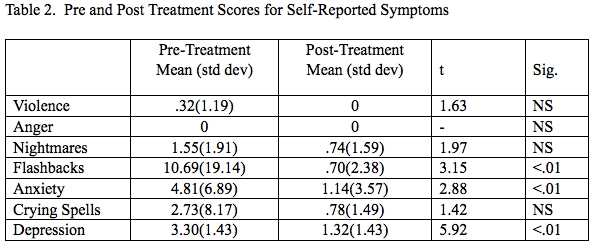
The first hypothesis of this study was that the T.R.U. method would significantly reduce PTSD symptomatology. The range of frequency of anxiety attacks prior to treatment was 0-28 and was 0-21 after treatment. The range of frequency of flashbacks prior to treatment was 0-84 and was 0-14 after treatment. Prior to treatment, subjects self-reported significantly higher frequencies of anxiety attacks per week (M=4.81, SD=6.89) than they did following the treatment (M=1.14, SD=3.57), t=2.88, p<.01. Subjects also reported significantly greater frequency of flashbacks prior to treatment (M=10.69, SD=19.14) than they did post-treatment (M=.70, SD=2.38), t=3.15, p<.01. Pre-treatment levels of depression were rated at a higher level (M=3.30, SD=1.43) than they were following treatment (M=1.32, SD=1.43), t=5.92, p<.01. Although the frequency of nightmares and crying spells was reduced after treatment, this was not to a statistically significant degree (see Table 2).
Table 2. Pre and Post Treatment Scores for Self-Reported Symptoms
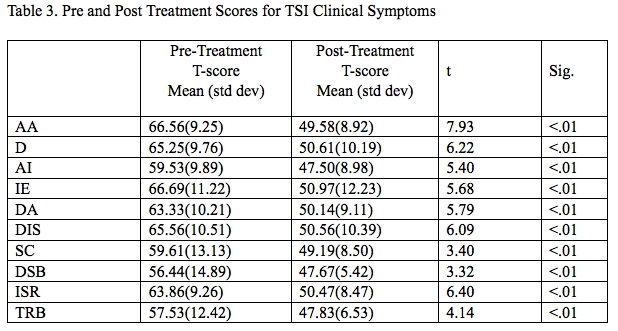
With regard to the objective self-report measure, the TSI, subjects experienced a reduction in post-traumatic symptomatology. Each of the clinical scales on the TSI was significantly reduced from pre-treatment to post-treatment (see Table 3). Comparing the results by the two clinicians, the first clinician, the creator of the T.R.U. method, had similar results as the whole sample. The second clinician had a significant reduction in her subject's symptoms for all clinical scales with the exception of Anger/Irritability (AI), Sexual Concerns (SC), and Dysfunctional Sexual Behavior (DSB). The first group who started the treatment program immediately also yielded the same results as the whole sample, as did the second group who waited one month before beginning treatment although with the exception of the DSB clinical scale.
Table 3. Pre and Post Treatment Scores for TSI Clinical Symptoms
Discussion
The findings of this study indicate that the T.R.U. method is effective in reducing the symptoms commonly associated with post traumatic stress disorder. This method significantly reduced the frequency of flashbacks and anxiety attacks. Clinician rated level of depression was also significantly reduced after treatment. All of the clinical symptom scales on the TSI were significantly reduced after treatment.
These findings also indicate that another therapist can administer the T.R.U. treatment with significant results. Future research should include a larger number of subjects conducted by another therapist.
Although there were thirty-seven individuals in the final analyses, future studies should include a larger sample size. The TSI is a psychometrically sound instrument yet, it has a large number of variables (10 clinical scales). It is suggested that a power analysis be conducted to determine the number of subjects needed to conduct a study using the variables included herein. This would reduce the likelihood of error and threats to the validity of the study.
